Introduction
Erectile dysfunction (ED) following prostate cancer treatment remains one of the most distressing complications for patients and their partners. For men undergoing definitive radiotherapy, whether external beam radiotherapy (EBRT) or brachytherapy, sexual function often deteriorates within months to years of treatment. Reported rates of moderate to severe ED range from 40% to 70% at 2 years, with considerable variability depending on baseline function, comorbidities, and treatment technique.
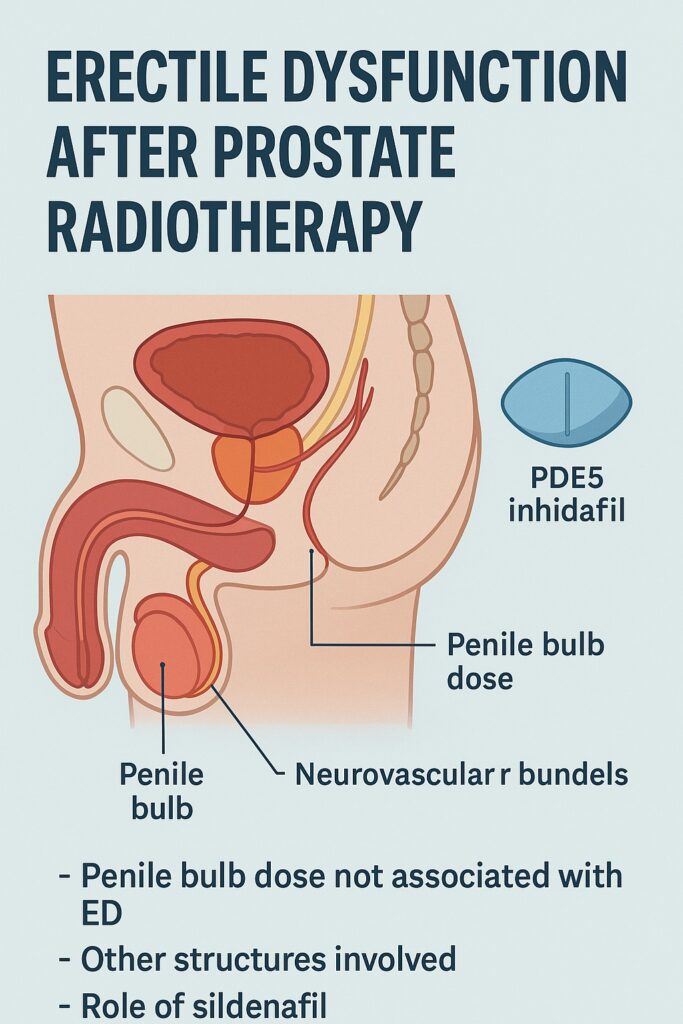
For years, radiation oncologists and urologists have debated which anatomical structures must be spared to preserve erectile function. The penile bulb, a midline structure at the base of the penis easily visualized on imaging, was thought to be particularly important. Early studies suggested that higher radiation doses to the penile bulb correlated with higher rates of ED, leading to treatment planning guidelines emphasizing penile bulb sparing.
However, newer prospective analyses challenge this dogma. A secondary analysis of a large randomized trial, published in Clinical and Translational Radiation Oncology in 2018, concluded that penile bulb dose was not significantly associated with ED at 18 months post-radiotherapy. This finding has profound implications: perhaps we have been targeting the wrong surrogate, and true culprits lie elsewhere.
This article explores the evolving science behind post-radiotherapy ED, examining anatomical, physiological, and psychosocial contributors. It also reviews pharmacological solutions such as sildenafil, as well as rehabilitation strategies aimed at preserving quality of life for prostate cancer survivors.
Radiotherapy and the Male Pelvis: Mechanisms of Injury
Radiotherapy achieves cancer control by delivering ionizing radiation to malignant tissue. Yet, collateral damage to adjacent structures is inevitable. The pelvis contains a tightly packed constellation of nerves, vessels, and muscles essential for erectile function, and each is vulnerable to radiation.
At the vascular level, radiation induces endothelial damage, intimal thickening, and fibrosis within the cavernosal arteries and penile vasculature. Reduced nitric oxide bioavailability further compromises smooth muscle relaxation, impairing blood inflow necessary for erection. Over time, this manifests as a vascular form of erectile dysfunction analogous to atherosclerosis, but accelerated by radiation injury.
At the neural level, the neurovascular bundles running posterolateral to the prostate are exquisitely sensitive. Even with advanced conformal techniques such as IMRT (intensity-modulated radiotherapy), incidental dose to these bundles occurs. Neural injury may lead to delayed or incomplete erectile response, compounding vascular compromise.
Finally, cavernous smooth muscle may undergo direct fibrosis and apoptosis, reducing compliance and veno-occlusive function. This prevents the penis from trapping blood effectively during tumescence, a mechanism central to durable erections. Together, these insults—vascular, neural, and muscular—create a multifactorial pathophysiology distinct from purely psychogenic or age-related ED.
The Penile Bulb Hypothesis: Origins and Challenges
The penile bulb, anatomically the posterior expansion of the corpus spongiosum, is readily visible on CT and MRI, making it a convenient surrogate for erectile structures during treatment planning. Early retrospective series suggested correlations between higher mean penile bulb doses and poorer erectile outcomes. This led to QUANTEC (Quantitative Analyses of Normal Tissue Effects in the Clinic) recommendations that planners should minimize dose to the penile bulb whenever possible.
However, the biological plausibility of the penile bulb as a causal structure has always been tenuous. The bulb itself is not richly innervated by autonomic fibers nor central to penile rigidity. Instead, its function relates to urethral compression and venous outflow modulation. The real drivers of erections—the paired corpora cavernosa and the neurovascular bundles—are located more anteriorly and laterally, not within the bulb.
Subsequent studies questioned whether the observed correlations were spurious. High penile bulb doses often co-occurred with high doses to adjacent cavernous structures and neurovascular tissue. Thus, the bulb may have been acting as a dosimetric bystander—a surrogate marker of more relevant injury, rather than the cause itself.
The 2018 secondary analysis of a randomized trial provided the clearest evidence yet: no statistically significant association between penile bulb dose and ED at 18 months. This calls for a shift in perspective, away from bulb-centric planning towards a more holistic consideration of true erectile anatomy.
Evidence from Clinical Trials: Sorting Signal from Noise
Prospective trials evaluating erectile outcomes after prostate radiotherapy have historically been hampered by heterogeneity in definitions, measurement tools, and patient selection. Some rely on physician-reported toxicity scales, others on patient questionnaires such as the International Index of Erectile Function (IIEF). This variability complicates meta-analyses.
The 2018 study reanalyzed data from a randomized controlled trial of dose-escalated EBRT. Patients were stratified by radiation dose to the penile bulb, and erectile function was assessed using validated questionnaires. At 18 months, the incidence of moderate-to-severe ED was high overall, but no correlation emerged between penile bulb dose and erectile outcomes. These findings held even after adjusting for baseline function and comorbidities.
Other studies corroborate these results. For instance, a Dutch multicenter cohort using MRI-based contouring of erectile structures found stronger associations between dose to the crura and proximal corpora cavernosa than to the penile bulb. Similarly, sparing the neurovascular bundles during IMRT planning correlated with improved outcomes, reinforcing the idea that the bulb is not the critical player.
Together, these data suggest that while penile bulb sparing may be harmless, it should not be the primary focus of erectile preservation strategies. Instead, attention should be redirected to more biologically plausible structures.
Alternative Predictors of Post-Radiotherapy ED
If the penile bulb is exonerated, where should attention turn? Multiple structures and systemic factors emerge as more reliable predictors.
The neurovascular bundles appear paramount. Radiation-induced neuropathy impairs neurotransmitter release (notably nitric oxide) critical for initiating cavernosal smooth muscle relaxation. Even sub-lethal neural damage can delay or blunt erectile response.
The corpora cavernosa, especially their proximal segments and crura, demonstrate dose-response relationships with ED risk. Fibrotic remodeling of cavernosal smooth muscle and trabecular tissue impairs rigidity and veno-occlusion. Advanced imaging studies show dose to these regions correlates strongly with IIEF decline.
Systemic comorbidities—diabetes, hypertension, smoking—exacerbate vulnerability. Men with baseline vascular risk factors experience steeper declines, underscoring the interplay between treatment injury and pre-existing endothelial dysfunction. Age, unsurprisingly, compounds risk, with older patients less able to compensate physiologically.
Thus, the emerging consensus is that ED after radiotherapy is multifactorial, with the penile bulb a minor character at best. The stage is dominated by neurovascular bundles, cavernosal tissue, and systemic health.
Pharmacological Interventions: The Role of PDE5 Inhibitors
Enter sildenafil, the archetypal phosphodiesterase-5 (PDE5) inhibitor. By preventing breakdown of cGMP in cavernosal smooth muscle, sildenafil amplifies nitric oxide signaling, facilitating relaxation and blood inflow. In the setting of radiation-induced vascular and neural compromise, sildenafil often restores sufficient erectile response, though not universally.
Randomized controlled trials demonstrate that sildenafil improves erectile function in post-radiotherapy patients, though efficacy rates are lower than in men with psychogenic or mild vasculogenic ED. Response rates vary from 50–70%, reflecting residual capacity of neurovascular signaling. Patients with intact baseline function, fewer comorbidities, and lower cavernosal radiation dose respond best.
Other PDE5 inhibitors, such as tadalafil and vardenafil, show similar efficacy profiles. Daily low-dose tadalafil has also been explored as a “penile rehabilitation” strategy, aiming to preserve smooth muscle integrity through regular oxygenation and mechanical stretch. Early-phase studies suggest improved long-term outcomes compared to on-demand use, though definitive evidence is still awaited.
Sildenafil’s success in this domain underscores an important point: even when structural injury is unavoidable, pharmacological modulation of residual physiology can yield meaningful functional recovery.
Rehabilitation and Preventive Strategies
Beyond pharmacology, comprehensive rehabilitation programs aim to preserve erectile function proactively rather than reactively. The concept of penile rehabilitation, borrowed from post-prostatectomy care, is gaining traction in radiotherapy.
Vacuum erection devices (VEDs) provide mechanical stretch and oxygenation, mitigating fibrosis and hypoxia-induced smooth muscle loss. Regular use during and after radiotherapy may preserve long-term function, though adherence is often challenging.
Pelvic floor exercises and cardiovascular conditioning also play supportive roles, enhancing baseline vascular health and neuromuscular coordination. Lifestyle modification—cessation of smoking, improved glycemic control, weight management—cannot be overstated. Each reduces the compounding burden on irradiated vasculature.
Psychosexual counseling addresses the psychological dimensions of ED. Anxiety, depression, and relationship strain amplify physiologic deficits. Integrating couples-based counseling into survivorship care not only restores intimacy but also improves adherence to rehabilitation regimens.
Thus, optimal management of radiation-induced ED is multimodal, blending PDE5 inhibitors like sildenafil with rehabilitation devices, lifestyle optimization, and psychosocial support.
Clinical Implications and Future Directions
The dethroning of the penile bulb as a key predictor of ED invites a recalibration of treatment planning. Rather than focusing on bulb dose, planners should prioritize sparing of neurovascular bundles and cavernosal tissue when feasible. Advanced techniques such as MRI-guided contouring, proton therapy, and adaptive planning may enhance this precision.
Prospective trials should adopt standardized, patient-reported outcomes using tools like the IIEF, with long-term follow-up to capture delayed dysfunction. Integration of imaging biomarkers, such as diffusion tensor imaging of nerves or perfusion MRI of erectile tissue, could refine predictive models.
Pharmacologically, the next frontier may involve combining PDE5 inhibitors with novel agents targeting fibrosis, angiogenesis, or neuroprotection. Gene therapies restoring nitric oxide synthase function are under exploration. Meanwhile, ongoing trials will clarify whether early initiation of rehabilitation improves durable outcomes compared to delayed rescue.
Ultimately, the shift away from bulb-centric thinking highlights a broader truth: preserving quality of life in prostate cancer survivorship requires precision, proactivity, and personalization.
Conclusion
Erectile dysfunction after prostate radiotherapy is a multifaceted challenge. Once thought to hinge on penile bulb dose, contemporary evidence demonstrates this is not the decisive factor. Instead, attention must pivot to neurovascular bundles, cavernosal tissue, and systemic comorbidities.
Pharmacological solutions, led by sildenafil and other PDE5 inhibitors, offer meaningful though imperfect relief. Rehabilitation strategies extend this impact, emphasizing multimodal approaches. The future lies in more anatomically precise treatment planning, integrated rehabilitation, and novel biologic therapies.
That a once “lifestyle drug” like sildenafil is central to restoring intimacy after cancer treatment is both ironic and hopeful. In the end, survivorship is not only about years gained, but also about lives fully lived.
FAQ
1. Does sparing the penile bulb during radiotherapy prevent erectile dysfunction?
No. Recent prospective analyses show no significant association between penile bulb dose and erectile outcomes. More critical structures include neurovascular bundles and the corpora cavernosa.
2. How effective is sildenafil for men with ED after prostate radiotherapy?
Sildenafil restores erectile function in about 50–70% of men, with best results in those with mild baseline dysfunction and lower cavernous radiation doses. It is less effective in severe neurovascular injury.
3. Can erectile dysfunction after radiotherapy be prevented?
Partial prevention is possible with penile rehabilitation, early use of PDE5 inhibitors, lifestyle optimization, and precise radiotherapy techniques that spare erectile structures.
4. What is the future of research in this area?
Ongoing research focuses on advanced imaging for erectile structure sparing, early rehabilitation protocols, and combination therapies targeting vascular, neural, and fibrotic pathways.